

I Went Down an Egg Donor Research Rabbit Hole
Here's everything I learned about ovarian reserve and egg donors


Medical stuff makes me queasy. Organs, systems, processes — amazing, love them, but I don’t want to see it and I don’t want to know.
I *literally* passed out in the A&P lab in college.
And the female reproductive system specifically? As an incredibly gay man, believe me when I say my interest level has historically been zero.
Hard pass!
And then we decided to have a baby.
Suddenly I wanted to know everything. And the more I learned, the more fascinating it became. So today I’m sharing what I’ve learned about the egg donation process — what to look for medically in a donor, what the science actually means, and why any of it matters.
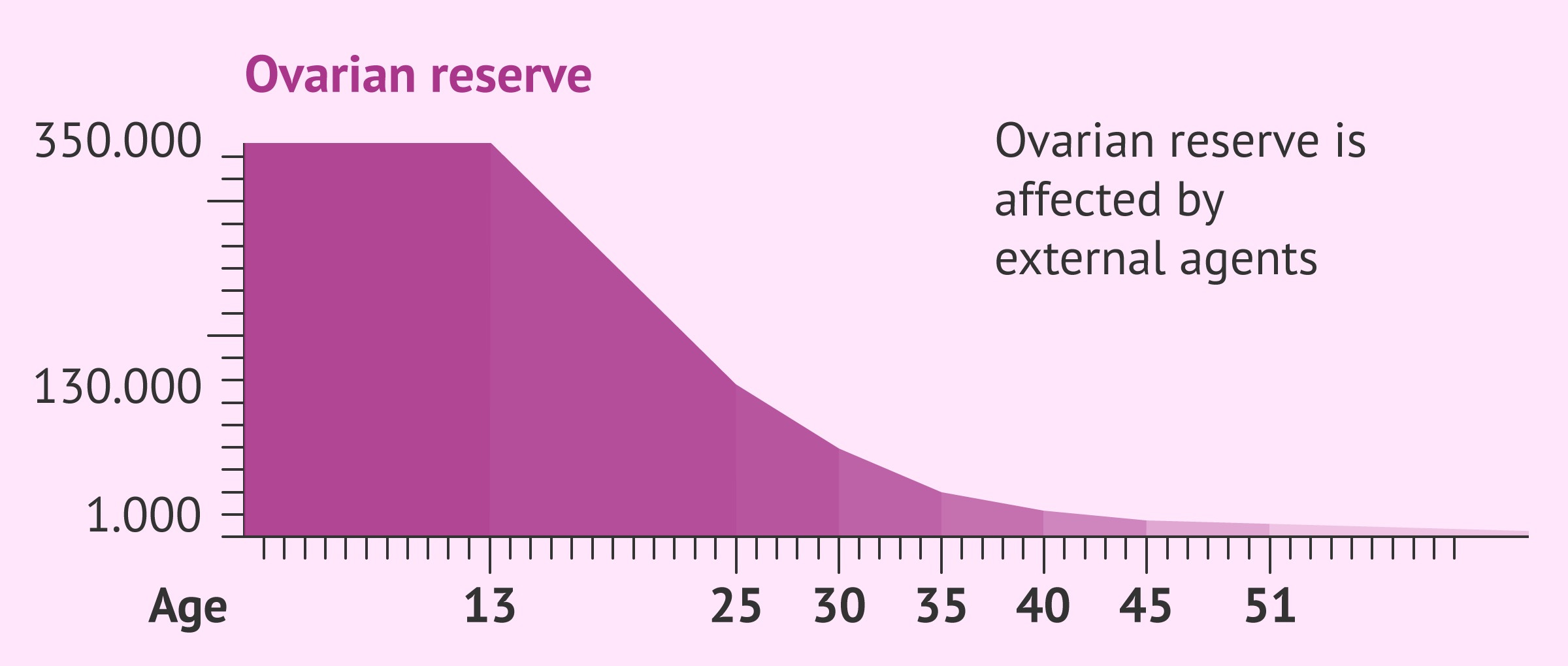
Let’s start at the very beginning: eggs are not infinite.
Women are born with all the eggs they will ever have, and the supply declines steadily over time. Not just through ovulation, but through a natural process called atresia, where follicles die off without ever maturing. Of the hundreds of thousands of eggs present at birth, only around 300 to 400 will ever actually ovulate. The rest are quietly lost along the way, until eventually — menopause.
Ovarian reserve: the most important thing I learned
Because eggs are finite, doctors have ways of measuring how many a woman has left and how well her ovaries are likely to respond when stimulated. This is called ovarian reserve. It turns out that when you’re searching for an egg donor, ovarian reserve is the single most important thing to understand, because it tells you what you can realistically expect from a cycle.
There are two key measurements that together paint the picture: AMH and AFC.
AMH: the hormone that estimates the pool
AMH stands for Anti-Müllerian Hormone. It’s produced by the small follicles in the ovaries, and a blood test measures how much of it is circulating in the body. The higher the AMH, the more active follicles there are, and the more eggs are likely to develop when the ovaries are stimulated. Think of it as a measure of how responsive the ovaries are likely to be.

Here’s what the numbers mean:
Below 1.0 ng/mL — very low ovarian reserve
1.0 to 1.9 ng/mL — low-normal, may have a modest response to stimulation
2.0 to 3.9 ng/mL — normal range for a healthy, fertile woman
4.0 to 6.8 ng/mL — high-normal, typical of a strong responder, often seen in women under 30
Above 6.8 ng/mL — very high, which can sometimes signal a risk of PCOS (Polycystic Ovary Syndrome) and overstimulation
For egg donors, clinics typically look for AMH above 2.0 ng/mL. An exceptional donor usually has AMH above 4.0 ng/mL, sometimes higher, which suggests her ovaries are likely to respond generously to stimulation and produce a strong number of eggs.
AFC: the ultrasound that counts what’s actually there
AFC stands for Antral Follicle Count. Where AMH measures follicle activity through a blood test, AFC puts eyes on it directly. A fertility doctor uses a transvaginal ultrasound to physically count the small resting follicles visible in both ovaries at that moment. Each follicle has the potential to contain a mature egg once stimulated.
A typical AFC is somewhere between 10 and 20 follicles across both ovaries. An exceptional donor often has an AFC of 25 or higher, which is a strong indicator that her ovaries will respond well to stimulation.
Doctors look at AMH and AFC together — along with the donor’s age — to build a complete picture of what to expect.
No single number tells the whole story, but together they’re a reliable preview.
")
So how do we actually use this to choose a donor?
Before we can answer that fully, we’ll need to talk through our family building goals with our doctor — specifically, how many children we’re hoping to have and how many embryos we’ll likely need. That conversation will determine how many mature eggs we need to retrieve, which will help us identify a donor whose AMH and AFC suggest she can realistically deliver that number.
Here’s what typical egg yields look like for young, healthy donors:
A typical donor cycle retrieves somewhere between 15 and 25 mature eggs
Donors aged 25 to 29 average around 18 mature eggs per cycle
Donors aged 30 to 35 average around 16 mature eggs per cycle
An exceptional donor in ideal conditions can yield 25 or more
Not all retrieved eggs will fertilize, and not all fertilized eggs will develop into viable embryos — so there’s always some math involved, and some buffer required. (I’ll share more about that in a future post!)
One thing to note: donors with exceptional AMH and AFC numbers often have higher compensation rates. Higher ovarian reserve generally means a more predictable cycle and a better chance of getting the number of embryos you’re hoping for. 1 (See footnote)
FAQ: the questions I had that you might have too…
Does donating eggs speed up menopause?
Nope! Not at all, actually. In a normal cycle, the body recruits a whole group of follicles each month, but only one actually matures and gets released. The rest quietly disintegrate. Stimulation rescues those follicles that would have been lost anyway and gives them a chance to mature. The eggs retrieved are eggs her body was going to waste that month regardless, so IVF doesn’t pull from her future supply. Menopause timeline stays the same!
Will the donor still get her period that month?
Mostly no… at least not on her usual schedule. The stimulation process temporarily overrides her natural cycle. She’ll likely have some bleeding after the retrieval as her body resets, but it won’t be a typical period. Her cycle usually returns to normal within four to six weeks.
Why are these numbers so different from what I’ve heard about IVF?
Since sharing our journey, so many women have generously let me into their own IVF experiences, and I feel genuinely privileged to have heard them. One thing I noticed is that egg yields varied wildly, and now I understand more about why.
Many people who pursue IVF for infertility have low AMH and AFC — diminished ovarian reserve is often part of why conception has been difficult in the first place. Fewer active follicles means fewer eggs retrieved, which is why yields for someone doing IVF with their own eggs can look very different from what I’m describing here. If you’ve been on that road, I want to acknowledge how hard that is. </3
On the other end, some women with PCOS have very high AMH and retrieve a large number of eggs — but because of hormonal imbalances, fewer of those eggs may be mature or viable. More isn’t always better.
Our situation is different because our egg donor is a young, healthy, pre-screened woman selected specifically for her strong ovarian reserve, not too low, not too high.
There’s so much to learn and so much to look forward to!
I’ll be doing a full post soon that walks through the entire IVF process from start to finish — what happens after the eggs are retrieved, how embryos are created and tested, and how our gestational carrier will fit into all of it. I’m so excited to learn and share more, and would love to answer any specific questions you might have!
In the meantime, I never thought I’d be the guy who could explain antral follicles at a dinner party…
But here we are!
Sources
Cofertility. “Choosing an Egg Donor: What AMH, AFC, and Age Can Tell You.” cofertility.com, 2025.
Cofertility. “How Many Donor Egg Cycles Does It Take to Have a Baby?” cofertility.com, 2025.
CNY Fertility. “Antral Follicle Count and IVF: What’s a Good Number.” cnyfertility.com, updated December 2025.
CNY Fertility. “Number of Eggs Retrieved in IVF: Average, Optimal, By Age.” cnyfertility.com, updated October 2025.
Athena Fertility. “How Many Eggs Can You Expect to Retrieve Based on Your AMH Level?” athena-fertility.com, 2025.
Cleveland Clinic. “IVF (In Vitro Fertilization): Procedure & How It Works.” my.clevelandclinic.org, updated January 2026.
Lin et al. “Factors Influencing Oocyte Yield and Embryo Quality in Donor IVF Cycles.” Frontiers in Endocrinology, 2025.
Quick note/correction: I originally had a line here that said, “The biology and the price tag are connected, which is its own conversation entirely.” It turns out I was wrong about that, and it was an assumption I made early on just from looking through donor profiles before fully understanding how the process actually works. I’ve removed the line because after talking more with clinics and egg donor agencies, I understand this differently now.
All eggs donors are choosing to donate their eggs. The compensation is not for the eggs themselves or “buying genetics.” The compensation is for everything the donor has to go through during the retrieval process — the time, travel, medications, injections, monitoring appointments, discomfort, recovery, etc. The donor also sets her own compensation expectations/rate through the agency process, meaning she decides what level of compensation would make undergoing all of that feel worth it to her.
Sorry for including something before that wasn’t totally accurate. I’m still learning a lot of this in real time and trying to share responsibly as I learn more. I’ll probably make a separate post at some point talking more about the ethics/questions around egg donation because my understanding of it has already evolved a lot!
I learned new things today! Also, PCOS was literally renamed just this last week as Polyendocrine Metabolic Ovarian Syndrome (PMOS)
Hey may I also share my personal experience? Well I’m going to only because it’s how we learn. I felt like a fraud walking through the fertility clinic doors. I had + pregnancy tests. I never wanted to see one again. I was one of the girls with great numbers and ranges. But we were there for Recurrent Pregnancy Loss. IVF was our only option if we wanted biological children without loss through spontaneous pregnancy. Wow! Writing that all out was heavy. I haven’t thought about it in years that way. Thank you spending the time researching and learning and sharing. We all only know what we know. xx